lesson 1: errors in diagnosis
Lesson 1: Errors in diagnosis
Treating the wrong case
(treating a contra-indicated cases)
Treating the wrong case (treating a contra-indicated cases)
- Root canal treatment should only be performed on teeth that can be predictably restored and have a reasonable prognosis.
- The AAE and ADA emphasize that endodontic treatment should only be done when properly indicated.
Code of nonmaleficence (do no harm) requiring clinicians to avoid unnecessary procedures that may harm the patient without benefit.
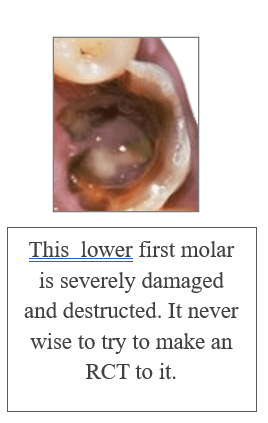
Non-restorable teeth (highly damaged teeth)
According to the American association of endodontists (AAE):
“Performing root canal treatment on non-restorable teeth is clinically inappropriate and ethically unacceptable.”
- A molar with <1 mm of remaining wall thickness or a deep vertical crack (fracture) is not suitable for root canal treatment.
- Performing RCT on such teeth will fail now or then.
Reasons we should not make RCT to a contra-indicated case
Poor long-term prognosis
A tooth with insufficient remaining structure cannot provide a tight coronal seal, making it vulnerable to reinfection, leakage, and treatment failure.
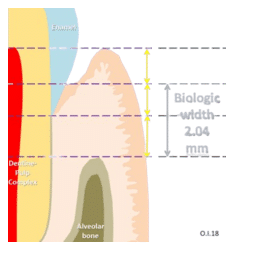
Violation of biologic width
If decay or fracture extends sub-gingivally or below the bone level, any attempt to restore the tooth might impinge on the periodontal attachment, leading to chronic inflammation and bone loss.
Unethical ( unnecessary treatment )
Performing RCT on a non-restorable tooth delays extraction, causes unneeded cost, discomfort, and may even worsen the surrounding bone and soft tissue status so harming the patient.
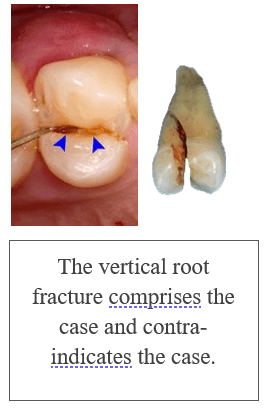
Vertical root fracture
A vertical root fracture is a longitudinal crack that extends from the root canal outward toward the periodontium and it cannot be repaired or sealed.
The crack allows bacteria, fluids, and debris to continuously enter the periodontal ligament space, even after root canal obturation, so re-infecting the root canal again.

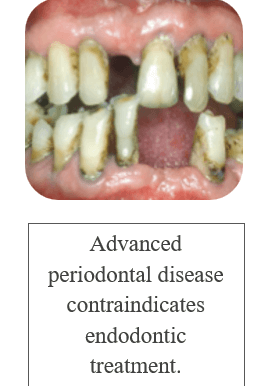
Advanced periodontal disease
- Periodontal pockets harbor anaerobic bacteria and biofilm.
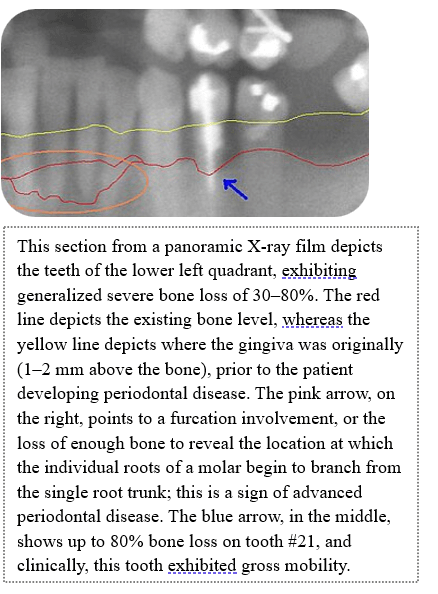
- In advanced periodontitis, there is severe bone loss around the tooth.
- This results in tooth mobility, deep pockets, and loss of attachment.
Even if RCT is done successfully, the tooth lacks bone support, and will eventually be lost due to periodontal failure (not endodontic failure).
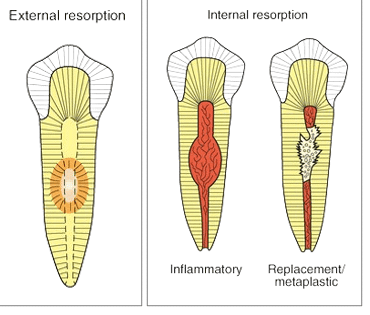
Extensive internal or external root resorption
Internal resorption: resorption begins within the pulp chamber or root canal system, typically due to chronic inflammation of the pulp. It leads to uniform widening inside the canal space.
External resorption: resorption occurs from the external root surface, involving the periodontal ligament and cementum, and may progress to dentin and even the pulp.
Reason it complicates the case
Resorptive processes often result in perforation.
The pulpal space opens into the periodontal ligament space, making endodontic seal unpredictable or impossible.
Non-repairable perforations
Perforation is a pathologic or iatrogenic communication between the root canal system and the external tooth surface (e.g., Periodontal ligament or oral cavity).
Perforation may occur in the floor of the pulp chamber, root canal wall, or furcation area.
RCT is contraindicated for Perforations when they are:
- Large in size.
- Located in non-accessible or non-sealable areas.
- Associated with severe periodontal damage.
- If delayed in their diagnosis.
A non-sealable perforation allows continuous leakage of bacteria and toxins into surrounding tissues, especially from saliva or periodontal pockets.
This leads to chronic inflammation, abscess formation, and failure of RCT.
Mobile teeth grade III
Grade III mobility: tooth shows greater movement in any direction, including vertical movement (Depressibility into the socket).
This indicates severe attachment loss, compromised alveolar bone support, and poor periodontal prognosis.
A grade III mobile tooth has severe periodontal destruction, often due to chronic periodontitis or trauma.
Even after successful RCT, the tooth cannot function due to the absence of supporting bone and ligaments.
Untreatable canal anatomy anomalies
Root canal systems with extreme, complex morphology that make proper cleaning, shaping, and obturation impossible.
Why contraindicated?
Certain anomalies (e.g. Dens invaginatus type III, fused roots, severe dilacerations, c-shaped canals) can prevent identification and access to all canals.
Extremely curved, narrow, or bifurcated canals increase the risk of file fracture, ledge formation, canal transportation, perforation.

Non-strategic tooth
Non-strategic tooth is a tooth that does not contribute to oral function, esthetics, or long-term prosthodontic or occlusal stability.
(tooth with no actual benefit)
This includes:
- Impacted or malposed third molars.
- Severely rotated or lingually displaced teeth.
- Teeth with no opposing tooth (non-functional occlusion).
- Teeth with poor prosthetic value (not needed for bridges or dentures).
- Supernumerary or retained deciduous teeth without orthodontic or esthetic value.
Why RCT is contra-indicated to non-strategic teeth?
No functional benefit.
Unjustified cost and time.
American dental association (ADA) says:
“Dentists should consider factors such as tooth restorability, periodontal support, and strategic importance before initiating endodontic therapy.”
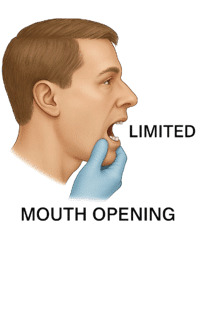
Severe gag reflex or limited mouth opening
Patients with a hypersensitive gag reflex:
- Cannot tolerate intraoral instruments, suction tips, or radiographic sensors.
- May experience nausea, vomiting, or even syncope.
- Rubber dam isolation becomes nearly impossible.
- Movement during canal instrumentation increases risk of file separation or perforation.
Limited mouth opening:
Inability to access posterior teeth (especially maxillary or mandibular molars).
Difficulty using handpieces, mirrors, endodontic files, apex locators.
Poor visualization = incomplete cleaning/shaping and failed obturation.