lesson 2: errors of access cavity
Lesson 2: errors of access cavity preparation
This lesson covers access cavity preparation errors, missed canals, access cavity shapes, common canal configurations, and Vertucci classification of root canal morphology.
Crown-root ratio
Crown-root ratio is the proportion of the tooth’s visible crown (above the alveolar bone) to the embedded root portion (within the bone).
1:1 (borderline crown-root ratio), should not decrease more than that.
A short root remaining in bone provides insufficient support.
After RCT, the tooth acts as a lever, increasing the risk of:
- Root fracture
- Dislodgment under occlusal forces
- Periodontal ligament trauma
Incorrect shape of access cavity
We will cover in detail:
- Reasons
- Correct access shapes
- Prevention
- Management
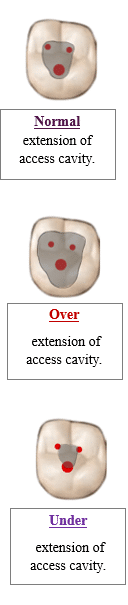
Over-extension of the access cavity
The access cavity becomes too wide (than necessary) or too deep.
Complications
- Difficulty in locating canals.
- Creating steps that make cleaning with files and obturation difficult.
- Unnecessary removal of tooth structure.
- Increased risk of perforation.
- Tooth weakening.
Under-extension of the access cavity
Under-extension of the access cavity occurs when the cavity is too small or shallow.
You fail to properly expose the pulp chamber and root canal orifices.
Complications
- Missed or blocked canal orifices.
- Difficulty locating all canals.
- Difficulty visualizing complex canal anatomy.
- Risk of reinfection due to incomplete cleaning and shaping.
Reasons, Prevention, Management
Failure to follow guidelines for specific teeth
Prevention
Study the anatomy of the tooth properly.
And
Follow standardized access cavity guidelines for each tooth.
Management
Take additional time to reshape and refine the cavity.
Inadequate control of bur angulation
Prevention
Use controlled and slow movements with the bur.
If you are a beginner: evaluate your progress during preparation by taking an x-ray while you are making access.
Anatomical variations
Prevention
Radiographs should be used to give you an idea about the anatomy of the tooth and possible variations.
CBCT is very useful for identifying complex anatomy.
Ultrasonic tips are helpful in locating hidden canals in a complex anatomy.
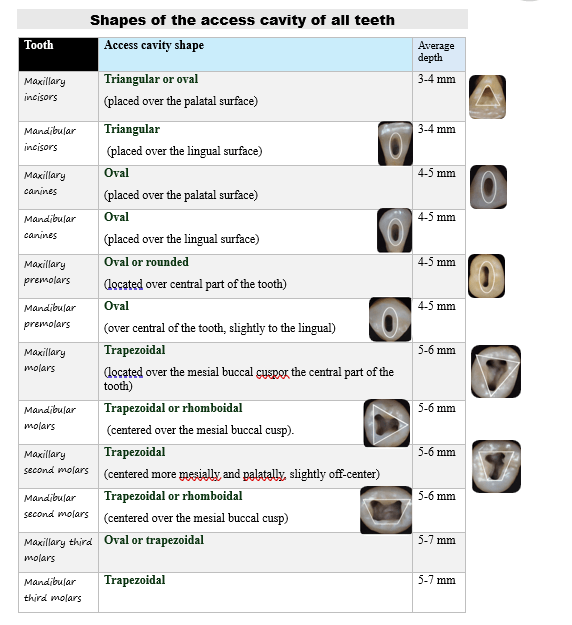
Shapes of the access cavity of all teeth
| Tooth | Access cavity shape | Average depth |
|---|---|---|
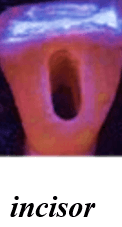
| Maxillary incisors | Triangular or oval (placed over the palatal surface)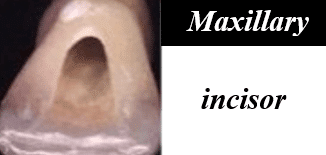 |
3-4 mm |
| Mandibular incisors | Triangular (placed over the lingual surface)
|
3-4 mm |
| Maxillary canines | Oval (placed over the palatal surface)
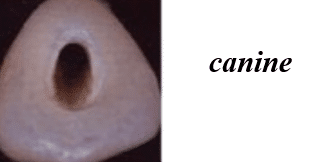
|
4-5 mm |
| Mandibular canines | Oval (placed over the lingual surface)
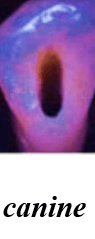
|
4-5 mm |
| Maxillary premolars | Oval or rounded (located over central part of the tooth)
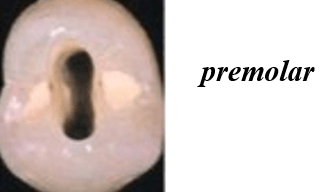
|
4-5 mm |
| Mandibular premolars | Oval (over central of the tooth, slightly to the lingual)
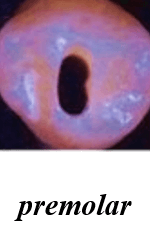
|
4-5 mm |
| Maxillary molars | Trapezoidal (located over the mesial buccal cusp or the central part of the tooth)
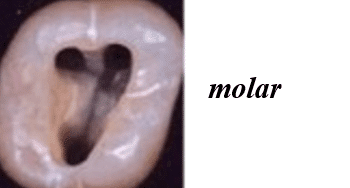
|
5-6 mm |
| Mandibular molars | Trapezoidal or rhomboidal (centered over the mesial buccal cusp)
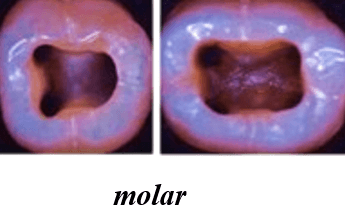
|
5-6 mm |
| Maxillary second molars | Trapezoidal (centered more mesially and palatally, slightly off-center) | 5-6 mm |
| Mandibular second molars | Trapezoidal or rhomboidal (centered over the mesial buccal cusp) | 5-6 mm |
| Maxillary third molars | Oval or trapezoidal | 5-7 mm |
| Mandibular third molars | Trapezoidal | 5-7 mm |
Missed Canals
| Possible reasons | Management |
|---|---|
|
Complex root canal anatomy Extra canals Lateral canals Accessory canals |
Re-evaluation If missed canals are suspected, consider taking additional radiographs from different angles, or utilize cone-beam C.T (CBCT). Use of magnification Dental loupes or operating microscopes are important for searching for small or hidden canals Re-access the tooth Reopen the access cavity to explore the canal system Use fine-sized burs and hand files to detect hidden canals Slightly expand the access cavity for better visibility Gentle negotiation Use small k-files Use ultrasonic tips To negotiate small canals. |
|
Inadequate access cavity If the access cavity is not large enough or is poorly positioned, it may prevent proper visualization or accessibility to all the canals. |
Re-access the tooth and slightly expand the access cavity for better visibility. |
|
Canal obstructions (debris, gutta percha, etc.) Canal obstructions caused by: Previous debris. Filling materials. Infected tissue. These can make it difficult to properly explore and negotiate all the canals. |
Re-evaluation, re-access, fine-sized burs, hand files, and gentle negotiation using small k-files and ultrasonic tips. |
If the access cavity is not large enough or is poorly positioned, it may prevent proper visualization or accessibility to all the canals.
ROOT CANALS
| Tooth type | Common number of roots & canals | Variations |
|---|---|---|
| Maxillary central incisor | 1 root 1 canal |
Rare: 2 canals (vertucci type II). |
| Maxillary lateral incisor | 1 root 1 canal |
Rare: 2 canals (type II). Dens invaginatus. |
| Maxillary canine | 1 root 1 canal |
Very Rare: 2 canals or bifurcation. |
| Maxillary first premolar | 2 roots 2 canals (one canal in every root) |
Rare: Single root with 2 canals. 3 canals. |
| Maxillary second premolar | 1 root 1 canal |
Rare: 2 canals, 2 foramina Rare: 3 canals |
| Maxillary first molar | 3 roots 3-4 canals |
2 canals in mb root (MB1 & MB2) Sometimes MB2 is hard to locate Very rare: 5 canals |
| Maxillary second molar | 3 roots 3 canals |
4 canals is less than upper 6. (MB2 common but less than 1st molar) Root fusion possible. |
| Maxillary third molar | Highly variable | 1–6 canals. Fused roots. Single or multiple canals. |
| Mandibular central incisor (1) | 1 root 1 canal |
Not common: 2 canals (labial + lingual) |
| Mandibular lateral incisor (2) | 1 root 1 canal |
Not common: 2 canals common |
| Mandibular canine (3) | 1 root 1 canal |
Rare: 2 canals May have 2 roots |
| Mandibular first premolar (4) | 1 root 1 canal |
Rare: 2 canals in one root (not common) or 2 roots, each root has one canal. (rare) |
| Mandibular second premolar (5) | 1 root 1 canal |
2 canals (not common) or 3 canals (rare). |
| Mandibular first molar (6) | 2 roots 3-4 canals |
4 canals (is less common than 3, but occurs alot) Mb, ML, DB, Dl Middle mesial canal (rare). |
| Mandibular second molar (7) | 2 roots 3 canals usually. |
C-shaped canal (rare). Middle mesial canal (rare). |
| Mandibular third molar (8) | Highly variable | 1–5 canals. Fused roots. Malformed roots. |
Vertucci classification of root canal morphology
- Type I (1–1): A single canal extends from the pulp chamber to a single apical foramen.
- Type II (2–1): Two separate canals leave the chamber and merge into one before the apex.
- Type III (1–2–1): One canal splits into two within the root, then rejoins into one at the apex.
- Type IV (2–2): Two distinct canals extend separately from chamber to apex.
- Type V (1–2): One canal leaves the chamber and divides into two separate canals near the apex.
- Type VI (2–1–2): Two canals merge in the root and then re-divide before the apex.
- Type VII (1–2–1–2): One canal splits, rejoins, and splits again before exiting the root.
- Type VIII (3–3): Three separate canals extend from the pulp chamber to three apical foramina.